

Extraocular muscles

Extraocular muscles are ones that make the eyeball itself move – and there is a lot going on to make that happen! In this post we’ll review the muscles, their attachments, innervations, actions, and testing procedures.
What are extraocular muscles?
Extraocular muscles are ones that originate from bony or fibrous connective tissue structures to insert onto the eyeball itself, thereby allowing us to look up, down, give someone the side-eye, and generally direct the gaze and orientation of the pupil.
There are six extraocular muscles proper - 4 that are straight so they are called "recti" and 2 that run on a diagonal so they are called "oblique." All six of these muscles must work together, and both sides in coordination with one another, so that the eyes look towards and focus on the same thing. Otherwise, our vision is blurred, doubled, or otherwise unclear.
Quick note, towards the end of this post I'll discuss an additional muscle that is not an "extraocular" muscle but one that raises the upper eyelid so we can see anything at all!

Superior rectus muscle
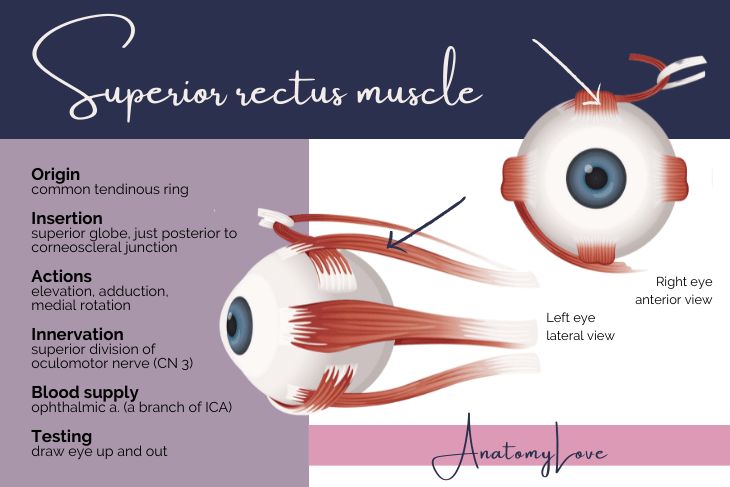
The superior rectus muscle is one of the 4 extraocular muscles that originate from the common tendinous ring (also called the annulus of Zinn) and insert onto the globe just posterior to the corneoscleral junction (pretty far anterior on the globe). It is on the "top" side of the eyeball, and straight in orientation, thus the same "superior rectus."
Innervation to the superior rectus muscle is through the superior division of the oculomotor nerve, cranial nerve 3.
Like the rest of the extraocular muscles, the blood supply to superior rectus is by way of the ophthalmic artery, a branch of the internal carotid artery (ICA).
The primary action of superior rectus is to elevate the eye so we look up. Secondary and tertiary actions are to adduct the eye and rotate it medially.
To test the superior rectus muscle, one must draw the eye out and up. This aligns the muscle fibers with the orientation of the gaze and more importantly, negates the muscle fibers of the other elevator of the eye, inferior oblique muscle.
Inferior rectus muscle
Take what is described above for the superior rectus muscle and apply it to a muscle on the lower part of the eye, instead. Importantly, the origin of inferior rectus muscle is still the common tendinous ring, or annulus of Zinn. The insertion is still on the globe just posterior to the corneoscleral junction, but on the inferior aspect of the eye.
Innervation to inferior rectus is the inferior division of the oculomotor nerve, cranial nerve 3, since it is in the lower orbit.
Blood supply is the ophthalmic artery, as for the rest of the extraocular muscles.
Given the position, the action of the inferior rectus muscle is to draw the eye down, or depress it. Additionally, inferior rectus can adduct and laterally rotate the eye.
As with the superior rectus muscle, testing of inferior rectus requires one to draw the eye laterally to line up the muscle fibers properly, and then have the patient look down, since the primary action is to depress the gaze. The eye in this position does not allow the other depressor, superior oblique, any line of pull on the globe which allows pure testing of inferior rectus.

Medial rectus muscle
The medial rectus muscle lies along the medial wall of the orbit, about half way between the roof and floor of the orbit. The insertion point is along the horizontal equator of the globe, about half way between the superior and inferior parts of the eyeball.
As with the other recti muscles, it originates from the common tendinous ring and inserts onto the medial aspect of the globe just posterior to the corneoscleral junction.
Innervation of medial rectus muscle is by way of the inferior division of the oculomotor nerve, cranial nerve 3.
The ophthalmic artery, a branch of the internal carotid artery (ICA), supplies medial rectus just like the rest of the extraocular muscles.
The medial rectus muscle explicitly adducts the eye, given the position of this muscle.
To test medial rectus, have the patient look left and right with the gaze in a neutral position (not elevated nor depressed). When the eye looks towards the midline, or the nose, that is testing the medial rectus muscle.

Lateral rectus muscle
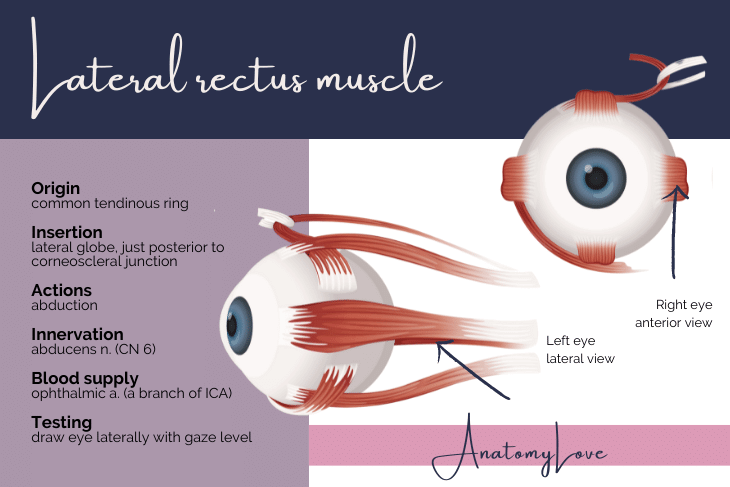
The lateral rectus muscle lies along the lateral orbit wall, about halfway between the floor and roof of the orbit. The origin of lateral rectus is the common tendinous ring, as for the other recti muscles. Similarly, it inserts onto the sclera just posterior to the corneoscleral junction, but on the lateral aspect and right at the horizontal equator of the globe.
Innervation of the lateral rectus is unique - the abducens nerve, cranial nerve 6, takes care of this muscle (and only this muscle).
Blood supply to lateral rectus still comes from the ophthalmic artery, a branch of the internal carotid artery (ICA).
The position and even the name of the nerve that innervates lateral rectus belies its action, which is to abduct the eye, explicitly.
Testing the lateral rectus muscle is done at the same time as medial rectus, which is done by having the patient look left and right, or towards and away from the nose, with the eyes otherwise level with the floor. When the eye is drawn towards the outside (abducted), the lateral rectus muscle is explicitly being tested.
Superior oblique muscle
Time for things on a diagonal!
The superior oblique muscle originates from the body of the sphenoid bone, near the apex of the orbit. Note that while the recti extraocular muscles originate from the common tendinous ring, the obliques have bony origins.
The course of the superior oblique muscle is unique in the orbit. From the sphenoid bone, the muscle belly runs anteriorly to find the trochlea, located in the superior-medial corner of the orbit (on the orbital plate of the frontal bone, just inside the medial superior orbital margin). The connective tissue sling of the trochlea allows the superior oblique to change direction. Muscle fibers course obliquely in a posterolateral fashion. The muscle passes deep to superior rectus muscle to insert onto the posterolateral portion of the eye, posterior to a vertical equator of the globe. This is an important feature that helps in understanding how the superior oblique does what it does (mentioned below!).
The innervation of the superior oblique muscle is the trochlear nerve, cranial nerve 4. That trochlea is therefore important both for changing the direction of superior oblique's muscle fibers, and in naming the nerve that supplies it (superior oblique is trochlear nerve's only target).
Blood supply to superior oblique is still the ophthalmic artery, a branch of the internal carotid artery, as with the rest of the extraocular muscles.
The action of the superior oblique is not as straight-forward as we might like but reviewing the course of muscle fibers as well as the insertion of the muscle will help. The anatomical action of the superior oblique muscle is to draw the eye "down and out" - so abduction, depression, and a little medial rotation, too. As I'll discuss below, if the muscles innervated by cranial nerve 3 are paralyzed, the eye is left in this position - down and out - because of the unopposed actions of superior oblique (and lateral rectus).
Testing the superior oblique requires that one pull the gaze of the eye into alignment with the oblique fibers of the muscle - those from the trochlea to the insertion. That means the eye must be drawn in, towards the nose, and then down. In this position, the only muscle that can depress the eye is superior oblique because the other depressor, inferior rectus, is not aligned with the line of sight and is thereby negated in action.

Inferior oblique muscle
Inferior oblique has a funky orientation, like superior oblique, but it is located in the lower part of the orbit, thus the name!
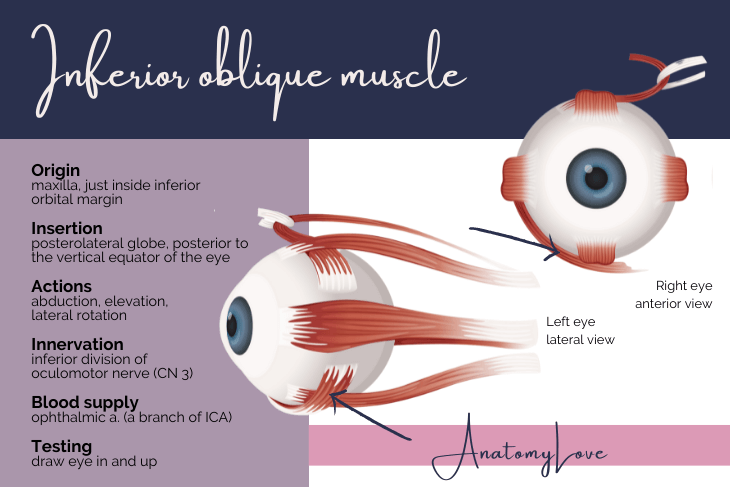
Like the superior oblique, inferior oblique has a bony origin. It arises from the orbital portion of the maxilla, tucked just inside the inferior-medial corner of the orbit, just inside the inferior orbital margin. This origin is very anterior in the orbit (and medial).
Also like the superior oblique, the inferior oblique inserts onto the posterolateral portion of the globe of the eye, very near the superior oblique muscle, actually. The direction of its fibers are therefore oblique (from anterior and medial to posterior and lateral). This orientation is key to understanding what the inferior oblique does (coming just below!).
The innervation to the inferior oblique is the inferior division of the oculomotor nerve, cranial nerve 3.
Blood supply is - you guessed it - still the ophthalmic artery, a branch of the internal carotid artery.
To test the inferior oblique, recall what we said for superior oblique - that the eye must be drawn into alignment with the muscle fibers. That means the eye must be drawn medially, towards the nose. Then, one must elevate the eye. In this position, inferior oblique is the only muscle that can elevate the eye because the other elevator, superior rectus, is not in alignment and thus negated in its action.
Review of extraocular muscle attachments
Rather than treating each extraocular muscle in turn, which I've done above, I also find it useful to group up factoids about the extraocular muscles to help identify patterns, similarities, differences, etc. Let's start with the attachments of these muscles:
Blanket rule: all recti muscles originate from the common tendinous ring and insert onto the sclera just posterior to the corneoscleral junction (pretty far anterior on the globe).
Blanket rule: both oblique muscles have bony origins (superior oblique from the body of the sphenoid bone, and inferior oblique from the maxilla) and insert near one another on the posterolateral portion of the globe (posterior to the vertical equator of the eye). Note that while the superior oblique muscle belly begins near the apex of the orbit, the important part of the muscle in terms of understanding its action is that portion from the trochlea to the insertion.

Review of extraocular muscle innervations
Again, I find it helpful to flip this information and look for patterns. Let's do that for innervations to extraocular muscles.
Blanket rule: superior oblique is innervated by the trochlear nerve, cranial nerve 4 - and that is the only muscle that nerve innervates, and it is named for the connective tissue pully by which superior oblique changes direction.
Blanket rule: lateral rectus is innervated by the abducens nerve, cranial nerve 6 - and that is the only muscle abducens innervates, named for the explicit and only action of it's one muscle, the lateral rectus.
Blanket rule: all other extraocular muscles are innervated by either superior division (superior rectus) or the inferior division (inferior rectus, inferior oblique, and medial rectus) of the oculomotor nerve, cranial nerve 3.

Review of extraocular muscle anatomical actions
In this section I'll review the anatomical actions of the extraocular muscles. That is, what they do based on their attachments, fiber orientation, and when acting alone (which nearly never happens). The next section will group up rules for testing these muscles.
Blanket rule: in addition to their obvious main actions (elevation via superior rectus, depression via inferior rectus, etc), recti muscles adduct the gaze - except for the obvious abductor, lateral rectus muscle.
Blanket rule: both oblique muscles abduct the gaze and move the eye opposite of their physical locations in the orbit (superior oblique depresses, inferior oblique elevates).

Below is a graphic summary of the anatomical actions of all the extraocular muscles, as described above. Note that this image relays their actions, not where to draw the eye when testing them (that is coming below!).

Review of extraocular muscle testing
Testing of the extraocular muscles feels counter-intuitive (at least to me!). Let's review the basic pattern to test them, a pattern you might be familiar with where the patient is asked to move their eyes and follow the finger of the examiner as they make an H in front of the patient's face.
Blanket rule: with the gaze neither elevated nor depressed, drawing the eye left and right (adducting and abducting) explicitly tests lateral rectus (abduction) and medial rectus (adduction) muscles; this is the cross bar of the H pattern.
Blanket rule: when the gaze is drawn towards the outside of one eye (abducted on one side, adducted on the other) and then elevated, the muscle being tested is the superior rectus while drawing the eye down (depression) in that position tests inferior rectus muscle.
Blanket rule: when the gaze is drawn towards the inside of one eye (adducted on one side, abducted on the other), with the eye now towards the nose, the examiner will again ask the patient to look up (testing inferior oblique) and then down (testing superior oblique). In this orientation the fibers of the oblique muscles are aligned with the direction of gaze, and deliberately NOT in line with the fiber orientation of any rectus muscle.

I put together a few flashcards of these "blanket rules" for eye muscle factoids. Flip through them below!
Levator palpebrae superioris muscle
Full disclosure, levator palpebrae superioris muscle is not an extraocular muscle, per se, but it is required in order to elevate the eyeLIDS to see anything at all.
The levator palpebrae superioris has a bony origin (sphenoid bone, again) but it inserts onto the upper eyelid at the superior tarsal plate - a connective tissue pad that gives the upper eyelid a bit of structure (rather than be a flap of skin and conjunctiva).
When I am in the lab with students I take care to remind them that when we do orbit dissections that require a superior view, as they nearly always do, it is the levator palpebrae superioris muscle that appears first (it is most superior in the middle of the orbit), not superior rectus. Superior rectus muscle is immediately underneath the levator palpebrae superioris muscle since superior rectus inserts onto the eyeball itself.
Interestingly enough, the levator palpebrae superioris is one of those unique muscles in the body that contains both skeletal and smooth muscle fibers. This is important in assessing the eyelid and how much it elevates (or not).
The skeletal muscle takes innervation from the superior division of the oculomotor nerve, cranial nerve 3. Being smooth muscle, the anterior extension of the levator palpebrae superioris muscle, called the superior tarsal muscle (in relation to the connective tissue plate of that name), is innervated by post-ganglionic sympathetic fibers that got there through the carotid sympathetic plexus (on the ICA).

The action of the levator palpebrae superioris is to elevate the upper eyelid, as the name suggests. Both the oculomotor nerve and the sympathetic fibers must be functioning properly to achieve a fully elevated eyelid.
When the levator palpebrae superioris muscle (and the nerves supplying it) is not functioning properly, it causes the upper eyelid to droop - a condition called ptosis - which ranges from mild to severe. Often, ptosis indicates a problem with the sympathetic innervation to the smooth muscle (superior tarsal muscle, the anterior extension of levator palpebrae superioris). If a patient is able to move their eyes around normally (indicating the oculomotor nerve is fine) but an eyelid is not fully elevating, this indicates a lesion of the sympathetic fibers to that muscle.
Ptosis is part of a suite of sympathetic features that manifest in the eye - Horner's syndrome. Before we get to how it shows up in the eye, it is important to mention that sympathetic innervation on the face causes sweating (all sweat glands are only innervated by the sympathetic autonomic system) and provides a sympathetic tone to blood vessel constriction (the lack of which produces a flushed face). Lack of sweating, or an overly dry face is called anhidrosis. The patient may also appear flushed on the same side. In the eye, sympathetic fibers dilate the pupil and fully elevate the upper eyelid through superior tarsal muscle. When the pupil is constricted it is called miosis. When the upper eyelid droops it is called ptosis. Typically these lesions are unilateral, given the course of sympathetic fibers onto the face and into the orbit. The lesion could arise from a tumor in the neck (often, a pancoast tumor of the apex of the lung), scar tissue, or generally anything that interrupts the path of these fibers. Horner's syndrome would therefore appear as lack of sweating (anhidrosis), a constricted and unresponsive pupil (miosis), and a droopy eyelid (ptosis) on only one side of the face and eye.

Downloadable diagram of extraocular muscles
I worked up a diagram to summarize the extraocular muscle anatomical actions, their innervations, and how to test them. A small version is shown below but if you'd like a PDF of that diagram, use the button!
