

Deep face and infratemporal fossa

The deep face and infratemporal fossae contain muscles of mastication and their blood supply, innervation, and venous return. The area is important for speech, chewing, and even salivation and taste, as several nerves move through this region to/from the oral cavity. The temporomandibular joint (TMJ) is also within this space.
Introduction to the deep face
The "deep face" is just that - the region of the face that is not easily seen from the outside but is still super important clinically because it houses muscles of mastication, their blood supply, innervation, and venous return, as well as many neurovascular structures important for proper articulation of speech, chewing food, and even salivation and taste. Because the muscles in this space move the jaw, a proper discussion of the temporomandibular joint (TMJ) is also in order.
Heads up - this post includes TWO downloadable drawings so be sure to grab them!
Okay, let's go!

Location of the "deep face," temporal, and infratemporal fossae
A quick way to conceptualize the "deep face" is to picture it deep to the mandible - but it is so much more than that, as we shall see! Let's back up to review that this region is usually subdivided into superior and inferior parts based on the zygomatic arch.
Temporal fossa
Temporal fossa is superior to the zygomatic arch while the infratemporal fossa is inferior to the zygomatic arch. Both fossae are deep to the arch itself. Let's review some of the boundaries for each fossa before going any further.
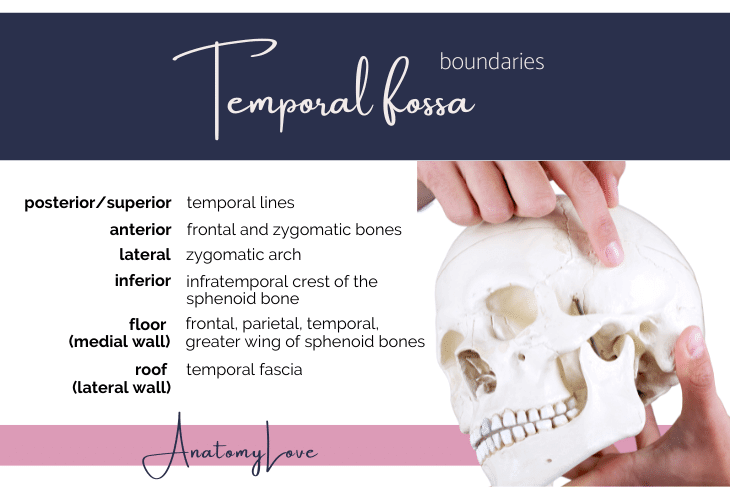
Temporal fossa boundaries:
Posterior/superior: temporal lines
Anterior: frontal & zygomatic bb.
Lateral: zygomatic arch
Inferior: infratemporal crest of sphenoid b.
Floor (medial wall): frontal, parietal, temporal, greater wing of sphenoid bb.
Roof (lateral wall): temporal fascia
Temporal fossa contents:
Temporalis muscle (the fan-shaped origin; note that the insertion reaches the infratemporal fossa)
Deep temporal nerves and arteries to the temporalis muscle
Temporalis fascia
The roof of the temporal fossa is the temporalis fascia and it deserves a quick mention.
For starters, the temporalis fascia is attached to the superior temporal line superficial to the temporalis muscle. It consists of two tough layers of fascia that run down to attach to both the deep and superficial sides of zygomatic arch inferiorly. The space between the fascial layers is filled with fat.
The fascia and fat protect the temporalis muscle. They also help to anchor the zygomatic arch from the strong downward force of the masseter muscle which is attached to the arch’s inferior border (because it is strong!).
Infratemporal fossa
The infratemporal fossa is what is usually meant by the "deep face" region. It is a bit of a small space packed with several muscle bellies, the nervous and arterial supply to those muscles, and even a few special players just moving on through (chorda tympani nerve, I'm looking at you!).
Infratemporal fossa boundaries:
Lateral: mandibular ramus
Medial: pterygoid muscles (lateral and medial)
Anterior: posterior aspect of maxilla bone (infratemporal surface of the maxilla)
Posterior: tympanic plate, mastoid & styloid processes of the temporal bone
Superior: inferior surface of the greater wing of sphenoid bone
Inferior: level of the angle of mandible

Let's do a quick list of the contents of the infratemporal fossa because this is what the rest of this post will be about:
Insertion of temporalis muscle
Medial and lateral pterygoid muscles
Maxillary artery
Pterygoid venous plexus
Mandibular division of the trigeminal nerve (CN V3) motor and sensory branches
Chorda tympani nerve (a branch of the facial nerve, CN 7)
Otic ganglion
Muscles of mastication
Mastication means chewing so the phrase "muscles of mastication" is just short-hand for grouping up the muscles that move the jaw. These muscles share origin from mesoderm of the first pharyngeal arch of a developing embryo. They also share motor innervation from the nerve to structures of the arch, the mandibular division of the trigeminal nerve (CN V3).
There are four primary muscles of mastication and a few small accessory muscles. Let's run through the main ones first!
Lateral pterygoid muscle
The lateralpterygoid muscle has two heads and two insertions. The superior head arises from the infratemporal crest and greater wing of the sphenoid to insert onto the joint capsule of the TMJ. The inferior head arises from the lateral surface of the lateral pterygoid plate to insert on the pterygoid fovea on the neck of the mandible.
When left and right lateral pterygoid muscles work together they depress the jaw and protract the mandible.
PRO TIP: the lateral pterygoid muscle is the only one to actively OPEN the jaw or depress the mandible. When only one side fires at a time it moves the jaw towards the opposite (contralateral) side.
This is important for grinding foods while masticating.
As with all the muscles of mastication, the motor nerve to the lateral pterygoid muscle is the mandibular division of the trigeminal nerve, or CN V3. It gets it's own named nerve, the "lateral pterygoid nerve" but it is more important to remember that the nerve comes from the trigeminal, the fifth cranial nerve.

Medial pterygoid muscle
Like the lateral pterygoid muscle, the medial pterygoid has two heads. The superficial head arises from the tuberosity of the maxilla (on the infratemporal/posterior surface of that bone) while the deep head arises from the medial side of the lateral pterygoid plate and the palatine bone (pyramidal process). Together, both heads of the medial pterygoid m. insert on the medial surface of the mandible, deep to the angle of the mandible.
PRO TIP: medial pterygoid is a mirror of the masseter muscle - they share orientation and actions (and cranial nerve innervation) but the masseter is on the superficial aspect of the mandibular ramus while the medial pterygoid is on the deep side. They make an "M&M" sandwich - the two muscles are the bread and the ramus of the mandible is the meat of the sandwich ;)
Since medial pterygoid muscle is a mirror of the masseter and their fiber orientations are similar, they both elevate and protrude the mandible when left and right sides work together. Acting unilaterally, each medial pterygoid muscle is able to move the jaw to the contralateral side as when chewing and grinding food (the same as lateral pterygoid does).
Because medial pterygoid muscle is a masticatory muscle it is innervated by the mandibular division of the trigeminal nerve like the others - and it does get it's own branch, the medial pterygoid nerve, but it is most important to remember cranial nerve five is the motor innervation to medial pterygoid.

Temporalis muscle
The temporalis muscle is a broad, fan-shaped muscle that covers most of the side of the head. It originates from the temporal fossa (covered above). In addition to the bony origin from the temporal fossa of the skull, superficial fibers of the temporalis take origin from the temporalis fascia covering this muscle (also see above). Fibers of the temporalis collect to insert onto the coronoid process of the mandible and the anterior border of the ramus of the mandible. It is very tendinous and tough at this location!
Because it originates superiorly and inserts inferiorly, the main action of the temporalis is to elevate the mandible. However, because fibers near the ear are nearly horizontal, temporalis can also retract the mandible.
The theme of motor innervation from the mandibular division of the trigeminal should feel familiar by this point. A pair of deep temporal nerves innervates the temporalis muscle.

Masseter muscle
The masseter muscle is a very powerful chewing muscle that originates from the zygomatic arch and inserts onto the ramus and angle of the mandible. Remember or read above about the "M&M" sandwich it forms with the mandible and medial pterygoid muscle since those two muscles have very similar fiber orientations, actions, and lie on superficial and deep sides of the mandible.
The masseter can close the jaw (elevate the mandible) and protrude it slightly.
As with the other muscles of mastication we've discussed here, the masseter muscle gets it's own nerve from the mandibular division of the trigeminal nerve - the masseteric nerve. To reach the deep side of this muscle that nerve and the artery that runs with it (a branch of the maxillary artery, discussed below) shoot the gap of the mandibular notch.

Other muscles that move the jaw
The four muscles covered above (lateral pterygoid, medial pterygoid, temporalis, and masseter) make up the "muscles of mastication" proper. However, a few other small muscles affect movements of the jaw and temporomandibular joint.
Suprahyoid muscles depress the mandible against resistance while the infrahyoid group is fixed (for review of those muscles see the post on anterior triangle of the neck)
Infrahyoid muscles fix or depress hyoid bone which helps depress the mandible, too
Platysma muscle can aid depression of the mandible against resistance (though mostly this muscle pulls down on the corners of the mouth and tenses skin of the neck); the post on the lateral cervical region covers platysma in detail)
Lesions of the mandibular division of the trigeminal nerve
Lesions of the trigeminal nerve deviate the jaw towards the lesioned side. This is because muscles that move the jaw tend to do so via left and right sides acting in unison. If left and right masseter, temporalis, and medial pterygoid muscles cannot elevate the jaw, or if only one side of the lateral pterygoid muscle is working properly, the jaw is pushed towards the weak side (where the nerve is lesioned).
Maxillary artery
The infratemporal fossa (aka: "deep face") includes a very large branch of the external carotid artery, the maxillary artery, which supplies the muscles of mastication, the temporomandibular joint, and even into the lower orbit, nasal cavity, and middle of the superficial face.
The maxillary artery is broken up into three portions relative to the lateral pterygoid muscle (FUN FACT: the maxillary artery may either be superficial OR deep to the lateral pterygoid muscle - in my experience it is a 50/50 shot as to which way it will go in any one person...and the branches from it are the same so the structures it supplies still get their blood...this is just a quirk of development of the face!).
Part 1 (lateral to the lateral pterygoid muscle) supplies: TMJ, ear, dura mater, portions of cranial nerves 5 and 7, mandibular teeth, and the chin
Part 2 (either directly deep or superficial to the lateral pterygoid muscle) supplies: the four muscles of mastication and the cheek
Part 3 (medial to the lateral pterygoid muscle and entering the pterygopalatine fossa) supplies: maxillary teeth, lower orbit and midface, the nasopharynx and sinuses, the palate, and the lower nasal septum

If you'd like a colored and labeled version of the drawing above, showing the maxillary artery, it's three parts, and all the branches - download your own copy below :D
Pterygoid venous plexus
Where blood goes it also needs to drain away - the deep face is no different! But, rather than one big vessel like we see in the maxillary artery, the veins in the deep face are more like a network laced throughout the infratemporal fossa. The pterygoid venous plexus does form a highly variable maxillary vein that is very short (a few millimeters). It collects blood from the plexus all throughout the deep face. Ultimately, the short maxillary vein drains into the large retromandibular vein located just deep to and posterior to the ramus of the mandible.
The plexus of veins in the deep face anastomoses with (connects to) the facial vein via the deep facial vein, as well as with the cavernous sinus (inside the cranial cavity) via emissary veins. Likewise, it is connected to the orbit through the infraorbital vein.
Mandibular division of the trigeminal nerve CN V3
The main nerve in the deep face is the mandibular division of the trigeminal nerve. A few other nerves move through this region too (branches of the facial nerve and the glossopharyngeal nerve, and we'll cover them below), but in the deep face CN V3 is key! This large nerve emerges from the middle cranial fossa into the infratemporal fossa by way of the foramen ovale in the base and greater wing of the sphenoid bone.
Unlike the other divisions of the trigeminal, CN V3 includes both motor and sensory fibers (the other branches of the trigeminal nerve are entirely sensory). CN V3 provides motor innervation to the primary muscles of mastication (temporalis, masseter, lateral pterygoid, medial pterygoid muscles) as well as accessory muscles of mastication (anterior belly of the digastric, mylohyoid, tensor veli palatini, and tensor tympani muscles). CN V3 is also carrying general sense afferent fibers from the lower cheek, mandibular teeth, anterior 2/3 of the tongue, the tympanic membrane, as well as most of the meninges. Let's run through the main branches of CN V3 here:
Auriculotemporal nerve
As it's name tells us, the auriculotemporal nerve of CN V3 moves laterally/transverse from the foramen ovale towards the ear and temple region of the superficial face. Of note for dissecting this nerve, it splits and surrounds the middle meningeal artery (a branch of the maxillary artery headed superiorly through the foramen spinosum). Auriculotemporal nerve provides general sensory afferent innervation to the auricle and temporal regions of the face (contributing to the CN V3 dermatome there) and also the temporomandibular joint.
Additionally, as we'll review below, the auriculotemporal nerve carries (as hitchhikers) general visceral efferent (GVE) parasympathetic fibers from CN IX, the glossopharyngeal nerve, to the parotid gland since it is near the ear and auriculotemporal nerve was headed that way anyway! To review innervation to the parotid gland, see the post on the superficial face and parotid region.
Inferior alveolar nerve
This nerve tells us it's distribution and targets in it's name - the inferior alveolar nerve enters the mandible to supply mandibular teeth and goes on to innervate skin of the chin, too. Inferior alveolar nerve enters the mandible through the mandibular foramen with an artery of same name (inferior alveolar artery, a branch of the maxillary artery). While within the body of the mandible the inferior alveolar nerve gives off dental branches that innervate mandibular teeth. Finally, what is left of the inferior alveolar nerve exits the mandible via the mental foramen as the mental nerve, providing sensory innervation to the skin over the chin, the lower lip, and gingiva of the mandible. Check out the post on the superficial face and parotid region to review the mental nerve and dermatomes of the face.
Another key relationship to know about the inferior alveolar nerve, is that right before it enters the mandible, a small nerve branches off - the nerve to mylohyoid - and travels along the inside aspect of the mandible within the mylohyoid groove until it reaches it's motor targets the mylohyoid muscle and the anterior digastric muscle...two muscles just under the chin. To review those muscles and other suprahyoid muscles of the neck, check out the post on the anterior triangle of the neck.
Lingual nerve
With a name like that, guess where the lingual nerve is headed...straight towards the tongue! Specifically, the lingual nerve provides general somatic afferent innervation (touch, pain, temperature) to the anterior two-thirds of the tongue. So, when you bite the tip of your tongue or burn it on a slice of pizza straight out of the oven (!), you can thank the lingual nerve, a large sensory branch of CN V3.
The lingual nerve carries, as hitchhikers, branches from another cranial nerve altogether - one that provides the special sense of taste (SVA fibers) from the anterior two-thirds of the tongue, along with parasympathetic motor innervation (GVE fibers) to salivary glands in the mouth - the chorda tympani nerve, a branch of the facial nerve. The submandibular ganglion, a parasympathetic ganglion that the facial nerve uses as a point of synapse to innervate the oral salivary glands, literally hangs off of the lingual nerve as it enters the back of the oral cavity. We'll review those relationships in detail below.
Buccal nerve
The buccal nerve provides general somatic afferent (GSA) innervation from the cheek and mucosa of the lower cheek inside the mouth, since "buccal" means "cheek!" One of the tips for identifying the buccal nerve of CN V3 is that it appears as if it emerges from between the two heads of the lateral pterygoid muscle. Oh! And always identify this nerve as the "buccal branch of the trigeminal nerve" because the facial nerve also has a buccal nerve but it is motor to facial muscles in this region and moves very differently. Review facial nerve branches in the post on the superficial face and parotid region.

Motor branches to muscles of mastication
As we reviewed above in the section on muscles of mastication, each muscle of mastication gets it's own branch from the mandibular division of the trigeminal nerve. Luckily, the nerves are named for the muscles they innervate:
Deep temporal nerves (always as least two) to the temporalis muscle
Masseteric nerve to the masseter muscle
Lateral pterygoid nerve to the lateral pterygoid muscle
Medial pterygoid nerve to the medial pterygoid muscle
Other relationships with the mandibular division of trigeminal nerve
As if learning branches of the mandibular division of trigeminal nerve wasn't exciting enough, parasympathetics and special sense fibers use branches of CN V3 to get to the parotid gland (CN IX fibers carried on auriculotemporal n.), sublingual and submandibular glands (CN VII fibers carried on lingual n.), and taste from the anterior 2/3 tongue (CN VII fibers carried on lingual n.).
As I reviewed in the post on the superficial face and parotid gland, the otic ganglion that the glossopharyngeal nerve uses to innervate the parotid gland is literally dangling off of the CN V3, just outside/inferior to foramen ovale. From the otic ganglion the post-ganglionic branches of CN IX use the auriculotemporal nerve of CN V3 to get to the parotid gland. Nice!
Another important relationship that I hinted at above, is between the lingual nerve (a sensory branch of CN V3) and chorda tympani nerve (a branch of the facial nerve, CN 7). Chorda tympani nerve emerges from the cranial cavity via the petrotympanic fissure which is located just posterolateral from foramen ovale. This is convenient because chorda tympani jumps into the epineurium of the lingual nerve to hitchhike with it towards the anterior two-thirds of the tongue. Like we just reviewed with the otic ganglion and CN V3 itself, the submandibular ganglion dangles off of the lingual nerve as that nerve enters the oral cavity. Chorda tympani carries two types of nerve fibers: pre-ganglionic parasympathetic (GVE, general visceral efferent motor fibers) from CN 7 (facial nerve) to the submandibular ganglion where they synapse and send post-ganglionic fibers to the sublingual and submandibular salivary glands (and mucosal glands) in the mouth. And, chorda tympani nerve also transmits special visceral afferent (SVA, special sense of taste) fibers from the anterior 2/3 of the tongue - remember that lingual nerve from CN V3 does general sense from that same region.
Temporomandibular joint
The temporomandibular joint (TMJ) is classified as a hinge-like condyloid synovial (diarthrodial) joint.
Bony components include the mandibular condyle/head and the mandibular fossa of the temporal bone. The lip of the mandibular fossa of the temporal bone includes the articular tubercle anteriorly. This bony bump helps guide and limit movements of the mandibular head in the fossa.
Ligamentous components include the joint capsule itself (since it is a synovial joint), which is attached to articular cartilage of the mandibular fossa of temporal bone and neck of the mandible. A fibrocartilaginous disc separates the cavity of the joint into superior and inferior spaces, each permitting different movements of the joint. A lateral ligament of the TMJ is a thickened area of the joint capsule, helping to minimize posterior dislocations of the joint. A few extrinsic ligaments of the TMJ further support the joint and mandible. The sphenomandibular ligament runs from the spine of the sphenoid to the lingula of the mandible. This ligament is the “swinging hinge” of the mandible, acting as a fulcrum and check ligament. The stylomandibular ligament runs from the styloid process to the inside angle of the mandible. It is a thickened portion of the connective tissue capsule that surrounds the parotid gland to provide minimal support of the mandible
When the mouth is closed the head of the mandible is retracted and sits within the mandibular fossae of the temporal bone. The chin is elevated by the natural tone of the retractors and elevators of the mandible. When we are sleeping or sitting upright the muscles can relax and gravity opens the mouth (lateral pterygoid muscle open the mouth actively, too). Opening the mouth moves the head of the mandible and the articular disc anteriorly (translation) towards the articular tubercle of the mandibular fossa. Translation without depression protrudes the chin forward. Pivot or small grinding movements result when only one side is protracted, causing the contralateral side to rotate while still retracted. To summarize, the TMJ is capable of the following movements:
Gliding (translation or protrusion/retrusion)
Flexion/elevation
Extension/depression
Rotation (pivot; only slight movements allowed)

Summary drawing of the neurovascular relationships in the deep face
I really like the deep face and understanding the structures that move through it. I developed a drawing packed with info and if you'd like to have a copy of the drawing you see below, click the DOWNLOAD button underneath it ;)

Bonus: this drawing is centered on the maxillary artery which spans the deep face and moves into the pterygopalatine fossa where it encounters branches of the maxillary division of the trigeminal nerve (CN V2). So, the drawing has a little "extra" besides deep face structures.
I hope you learned a little from this discussion of parts deep within your face - ones that allow you to chew and move the jaw, feel things from your lower teeth and chin, and even help the other nerves that allow tasting and salivation to get where they need to go.